CHRONIC GRANULOMATOUS DISEASE:
RADIOGRAPHIC MANIFESTATIONS
Brett D. Skidmore, M.D. and Gael J. Lonergan, M.D.
Wilford Hall Medical Center, San Antonio, Texas
INTRODUCTION
Chronic granulomatous disease (CGD) was first described in 1959 by Berendes, Bridges, and Good. These patients are prone to repeated infections and granuloma formation because of impaired leukocyte killing of engulfed microorganisms. Normal neutrophils and phagocytes oxidize glucose to form hydrogen peroxide; this helps eradicate vacuolized microorganisms. Patients with CGD, however, have insufficient hydrogen peroxide production. Also, some microorganisms (predominantly bacteria and fungi) produce catalase, which degrades hydrogen peroxide; these catalase-positive organisms are particularly virulent in the patient with CGD (1). Absence or deficiency of 4 separate proteins in the pathway of hydrogen peroxide production has been identified in CGD; one is x-linked recessive (60% of patients) and the other 3 are autosomal recessive (11).
Clinical presentation is in the first year of life, typically with recurrent lymphadenitis, pneumonia, and eczematous rash. Other manifestations include hepatosplenomegaly, urinary tract infection, cystitis, gastric antral thickening, and osteomyelitis. Bacteria and fungi that are especially problematic are S.aureus, E. coli, Pseudomonas, and Aspergillus. Diagnosis is confirmed with nitroblue terazolium (NBT), which is normally reduced (but not by CDG neutrophils) to blue formazan.
The cause of granulomata formation is unknown; they occur with and without proven infection and are more common in the x-linked recessive form. It has been postulated that they are a response to repeated foreign antigen exposure. This may explain the predilection of the gastric antrum, esophagus, lymph nodes and postoperative sites to sterile granuloma formation (8).
Chronic granulmatous disease is treated with antibiotics, steroids, and interferon, all of which are used both for treatment and prophylaxis. Prognosis previously was poor, with a 40% mortality rate by the age of 10. Recently, however, the 8 year survival rate has been estimated at 93% (8).
CGD:ABDOMEN
BACK TO RADIOLOGY CENTRAL RESOURCE
The abdomen is the most common site of involvement in CGD, most often manifest as antral disease. The patient may present with vomiting, abdominal pain, and weight loss. UGI examination demonstrates antral narrowing, usually circumferential, often with a sharp proximal margin (2). At US, the circumferential antral narrowing simulates hypertrophic pyloric stenosis. Endoscopy and biopsy in cases of antral disease have shown inflammatory changes but no bacteria. This suggests infection may not be the primary pathologic mechanism; rather, repeated antral exposure to foreign antigens may be the inciting event (5).
Other abdominal findings include colitis and perirectal disease, esophageal strictures (which appear to be primarily due to the inflammation of CGD and may not be infectious) (9), hepatosplenomegaly, hepatic and splenic granulomata, liver abscess (most often S. aureus), and mesenteric and retroperitoneal adenopathy.
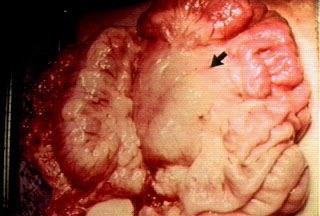
2 year old male underwent CT for abdominal pain and fevers. The enhanced CT image shows multiple nodular opacities in the mesentery (arrow). At surgery, multiple mesenteric granulomatous lymph nodes were found (arrow).
NEXT PAGE BACK TO RADIOLOGY CENTRAL RESOURCE
The lateral KUB shows abdominal ring-like calcifications in this 1 year old male with several month history of fever and irritability. The CT images demonstrate the calcifications in the mesenteric lymph nodes. Splenomegaly is also present. (Case courtesy of G. Hedlund, D.O.)

 NEXT PAGE
NEXT PAGE
BACK TO RADIOLOGY CENTRAL RESOURCE
An UGI series in a 3 year old male with solid food intolerance and vomiting demonstrates an elongated and narrowed antropyloric region, also seen on ultrasound (arrows). Marked antral wall thickening was confirmed by upper endoscopy.

NEXT PAGE
BACK TO RADIOLOGY CENTRAL RESOURCE
CT scan on a 1 year old male shows multiple low attenuation foci in the spleen, consistent with granulomata. (Case courtesy of G. Hedlund, D.O.)

CGD:CHEST
BACK TO RCR